Patellofemoral pain (PFP) is a common musckuloskeletal condition that presents as a poorly localized pain around or behind the patella (knee cap) during activities of patellofemoral joint loading (squats, stairs, running, lunges etc..)1. Clinically, our patients have a difficult time pin pointing the location of pain, describing it as a dull aching pain around the knee cap that can be sharper with strenuous activity. Positions of knee flexion (bend) are often more irritable than extension (straight leg) and swelling and localized tenderness is rare.
Patellofemoral pain has an annual prevalence of approximately 23% of adults and 29% of adolescents. Unfortunately, PFP tends to persist in about 50% of people, in some cases up to 20 years2. Pain and symptoms associated with PFP limit participation in daily and occupational tasks and reduce levels of physical activity. Most importantly, there is research that suggests that PFP may precede the onset of patellofemoral osteoarthritis3, which has no cure.
For the gym athlete PFP is most likely to present during squatting, lunging, running on treadmill or climbing the stair master. In order to properly manage these athletes it is important to have a thorough understanding of the joint forces that contribute to PFP.
What does the research say?
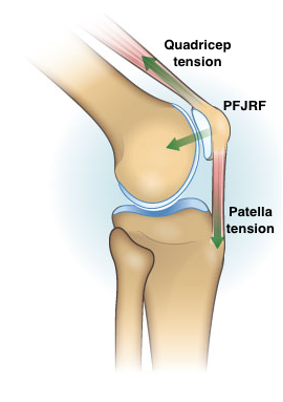
A recently published systematic review by Hart el al (2022)4 sought to identify patellofemoral joint reaction force (PFJRF) during everyday activities and therapeutic exercises. PFJRF is described as the reaction force caused by the tension in the quadricep muscle and patella tendon driving the patella into the surface of the distal femur4. Therefore, increase demand on the quadriceps (aka load) and increasing the degree of knee flexion (tension in the patellar tendon) can increase PFJRF and theoretically increase PFP symptoms.
A second metric that the Hart el al study investigated was Joint Contact Pressure Area aka how large a surface area is the PFJRF spread over. What they found is that the contact area between the patella and femur increased as knee flexion angles increased. This means that as the amplitude of PFJRF increases the contact surface also increases to better distribute this force. This would help us to explain why we can withstand large amounts of load with deeper knee flexion angles (think deep squats or lunges).
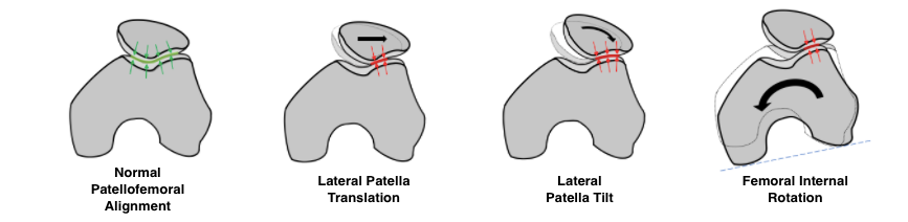
Interestingly enough, what the Hart et al study also highlights is the effect that altered kinematics such as hip adduction and femoral internal rotation have on the patellofemoral joint. Hip adduction and femoral internal rotation may lead to a shift in the location of the centre of contact pressure within the patellofemoral joint. This shift of contact pressure may lead to abnormally elevated contact pressures being applied to regions of cartilage that are not accustomed to high pressures and diminished pressures in regions that are accustomed to absorbing higher contact pressures. Both may trigger adverse changes in articular cartilage and contribute to the progression of patellofemoral osteoarthritis4.
Should I still squat with knee pain?
With the above biomechanical explanation we can now understand what contributes to increased patellofemoral joint reaction force (increased quadricep load and knee flexion angles) and what helps our patellofemoral joint to withstand these forces (larger contact surface through greater knee flexion angles, proper hip kinematics). So how can we apply this information to the gym athlete with knee cap pain?
Let’s consider a squatter that experiences right knee cap pain while squatting 225lb to a depth of 100 degrees of knee flexion. Given the above information we have a multitude of assessment and intervention strategies we can offer this person. Firstly, it is important to see the lifter perform their squat with the aggravating weight so that you can perform an analysis on squat technique under the appropriate load. During this assessment we would be looking for signs of altered kinematics (hip adduction, femoral internal rotation) that correlates to the lifter’s pain symptoms. If we identify these signs and are quite confident they relate to the lifter’s pain then we would put intervention strategies in place to educate and correct these altered mechanics.
While the lifter is working their way through their rehab exercises we also want to consider our knowledge of PFJRF and how we can keep our lifter squatting through their rehab plan. The two easiest variables to manipulate would be quad demand and knee flexion angle. Depending on the goals of the lifter we may modify one or both of these variables. For example, if the lifter’s goal is to maintain load we would modify the depth of squat using a bench or plyobox to reduce the knee flexion angles. If the lifter’s goal is to maintain squat depth through rehab than we would reduce bar weight and continue with depth squat as is. If neither modification reduces knee pain sufficiently we may use a combination of both modifications or switch to single leg loading.
Of course, the above rationale is a very biomechanical approach. There are other factors to consider such as training volume and frequency that may be leading to PFP. It is possible that by addressing these training errors we may not need to intervene with rehab exercises at all.
In summary, we know that patellofemoral pain effects up to a quarter of our adolescent and adult population and that these symptoms persist in about 50% of these individuals leading to reduced participation in daily tasks and physical activity levels2. It is critical that PFP be addressed and intervened as PFP has been associated with the onset of patellofemoral osteoarthritis3. In the gym population, PFP may be most prominent with squats, lunges, stair climber and running. An experienced Physiotherapist will be able to assess the biomechanics of the lifter as well as address any other training errors to create a rehab plan that keeps the athlete lifting through rehab and beyond!
Squat pain rehab in Kitchener-Waterloo
Modern Physiotherapy and Trainings Physiotherapist’s are experts in the management of knee injuries. We utilize a 4,500 sq ft gym and the most modern physiotherapy technology to assess and treat injury concerns. Book with us using the online booking link!

Citations:
1.Collins NJ, Barton CJ, van Middelkoop M, et al
2018 Consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain: recommendations from the 5th International Patellofemoral Pain Research Retreat, Gold Coast, Australia, 2017
British Journal of Sports Medicine 2018;52:1170-1178.
2.Smith BE , Selfe J , Thacker D , et al . Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PLoS One 2018;13:e0190892
3.Thomas MJ, Wood L, Selfe J, et al . Anterior knee pain in younger adults as a precursor to subsequent patellofemoral osteoarthritis: a systematic review. BMC Musculoskelet Disord 2010;11:201